Printable Vaccine Consent Form
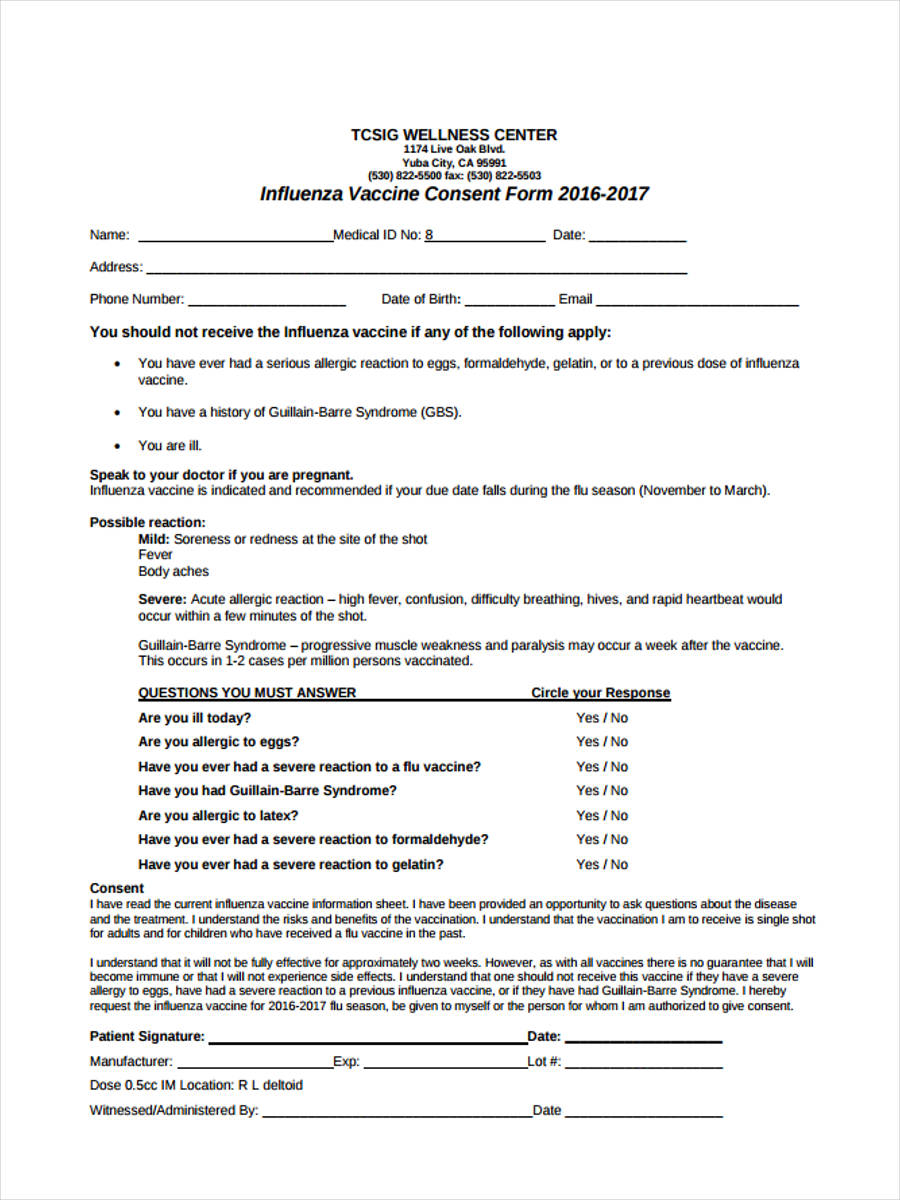
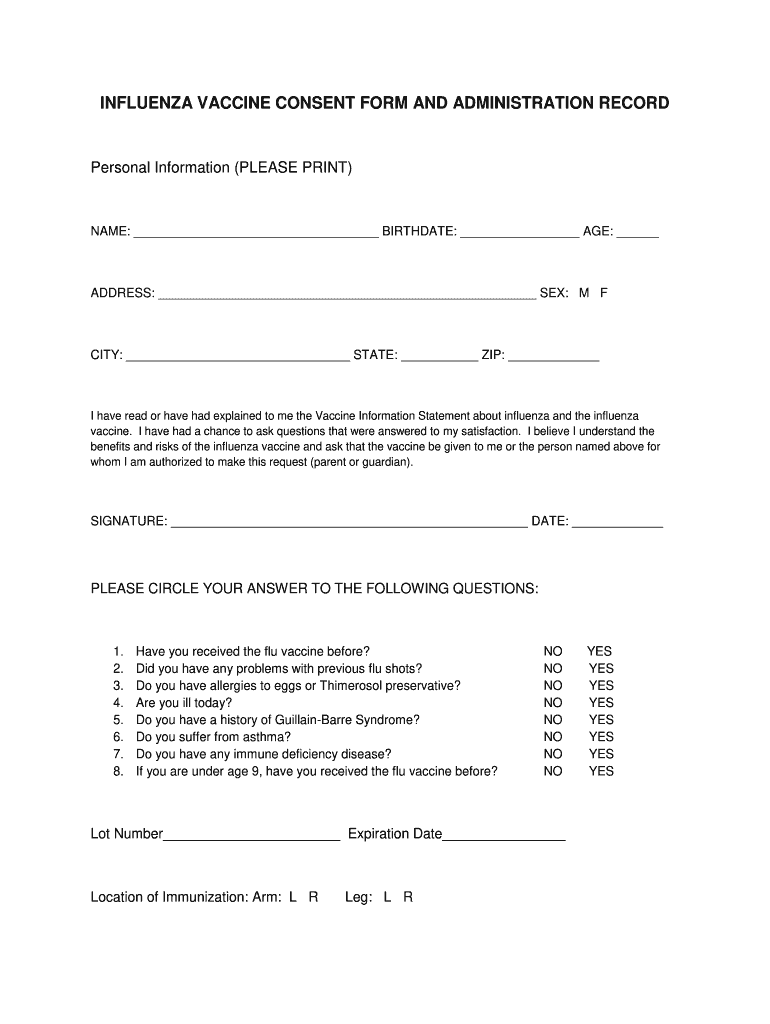
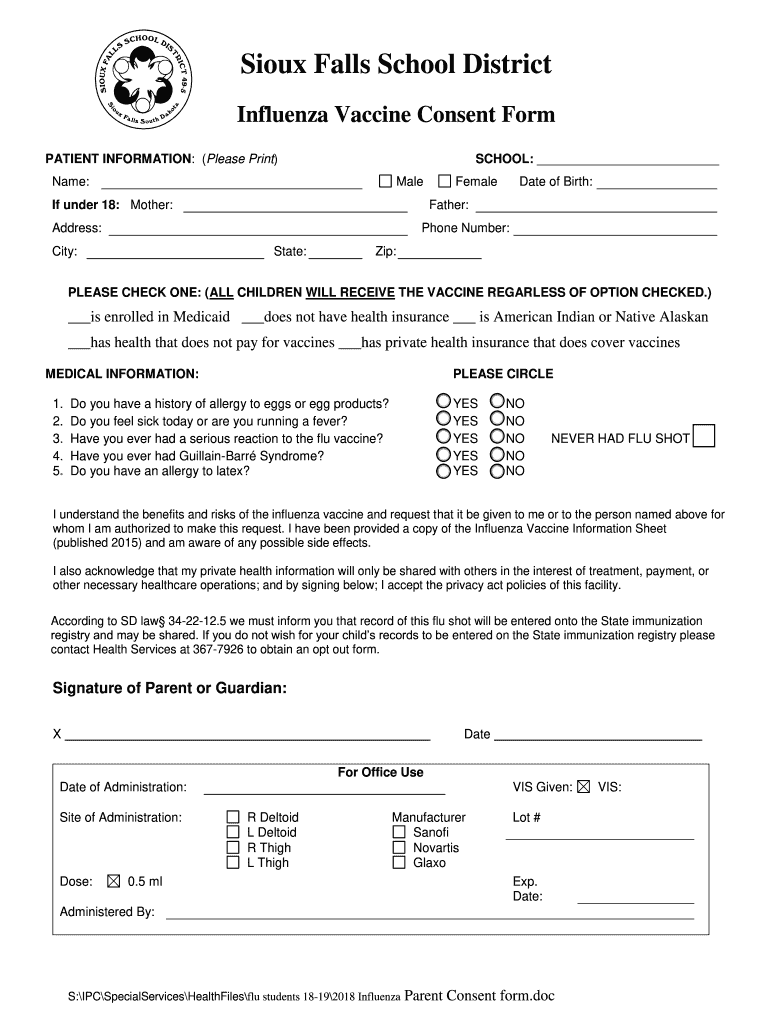
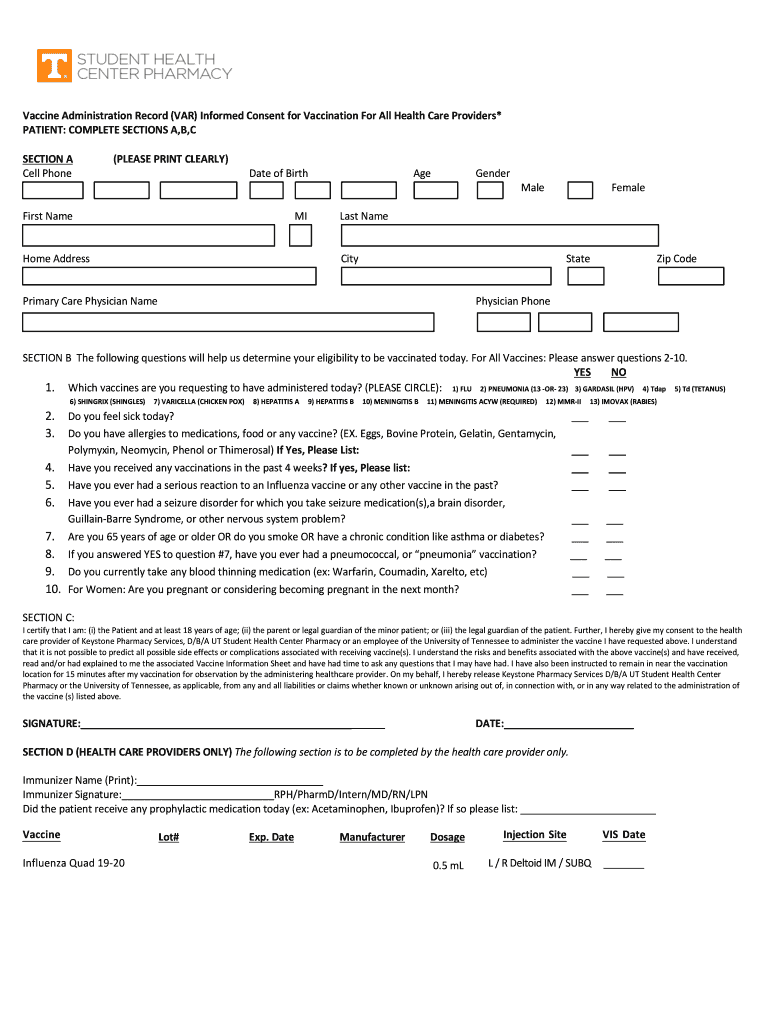
Printable Vaccine Consent Form - I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which. I request that the vaccine be given to me or to the person. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or. Vaccine administration record (var)—informed consent for vaccination answered. I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when. I understand the benefits and risks of the vaccine(s). Except for the last two (2). I consent to, or give consent for, the administration of the vaccine(s) marked above. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question.
By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or. Vaccine administration record (var)—informed consent for vaccination answered. I understand the benefits and risks of the vaccine(s). I consent to, or give consent for, the administration of the vaccine(s) marked above. Except for the last two (2). I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when. I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which. I request that the vaccine be given to me or to the person. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question.
I understand the benefits and risks of the vaccine(s). I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when. I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which. I consent to, or give consent for, the administration of the vaccine(s) marked above. Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or. I request that the vaccine be given to me or to the person. Except for the last two (2). Vaccine administration record (var)—informed consent for vaccination answered.
Printable Vaccine Consent Form Template Printable Forms Free Online
I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which. I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when. Vaccine administration record (var)—informed consent for vaccination answered. I request that the vaccine be given to me.
Printable Flu Vaccine Consent Form Template and guide airSlate SignNow
I request that the vaccine be given to me or to the person. Except for the last two (2). I understand the benefits and risks of the vaccine(s). I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when. Tell your vaccination provider about all your medical conditions, including.
Printable Flu Vaccine Consent Form Template Printable Word Searches
I request that the vaccine be given to me or to the person. I understand the benefits and risks of the vaccine(s). Except for the last two (2). I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when. I understand the benefits and risks of the vaccination(s) as.
Printable Flu Vaccine Consent Form Printable Word Searches
Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question. Vaccine administration record (var)—informed consent for vaccination answered. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or. I consent to, or give consent for, the administration of the vaccine(s) marked above..
Printable Flu Vaccine Consent Form Printable Word Searches
I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which. Except for the last two (2). I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when. Vaccine administration record (var)—informed consent for vaccination answered. I consent to,.
FREE 9 Vaccine Consent Forms In PDF Ms Word Printable Consent Form
I request that the vaccine be given to me or to the person. Except for the last two (2). Tell your vaccination provider about all your medical conditions, including if you answer “yes” to any question. I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which. Vaccine administration record.
Vaccine consent form pdf Fill out & sign online DocHub
By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or. Except for the last two (2). I understand the benefits and risks of the vaccine(s). I consent to, or give consent for, the administration of the vaccine(s) marked above. I request that the vaccine be given to me or.
Printable Flu Vaccine Consent Form Template Printable Word Searches
I consent to, or give consent for, the administration of the vaccine(s) marked above. I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when. Vaccine administration record (var)—informed consent for vaccination answered. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or.

Vaccine Consent Form 2 Free Templates in PDF, Word, Excel Download
I request that the vaccine be given to me or to the person. Vaccine administration record (var)—informed consent for vaccination answered. I understand the benefits and risks of the vaccine(s). I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when. I understand the benefits and risks of the.

COVID19 Vaccine Consent Form_spanish_moderna.docx Buena Vista County
I consent to, or give consent for, the administration of the vaccine(s) marked above. I request that the vaccine be given to me or to the person. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or. I understand the benefits and risks of the vaccine(s). I have been.
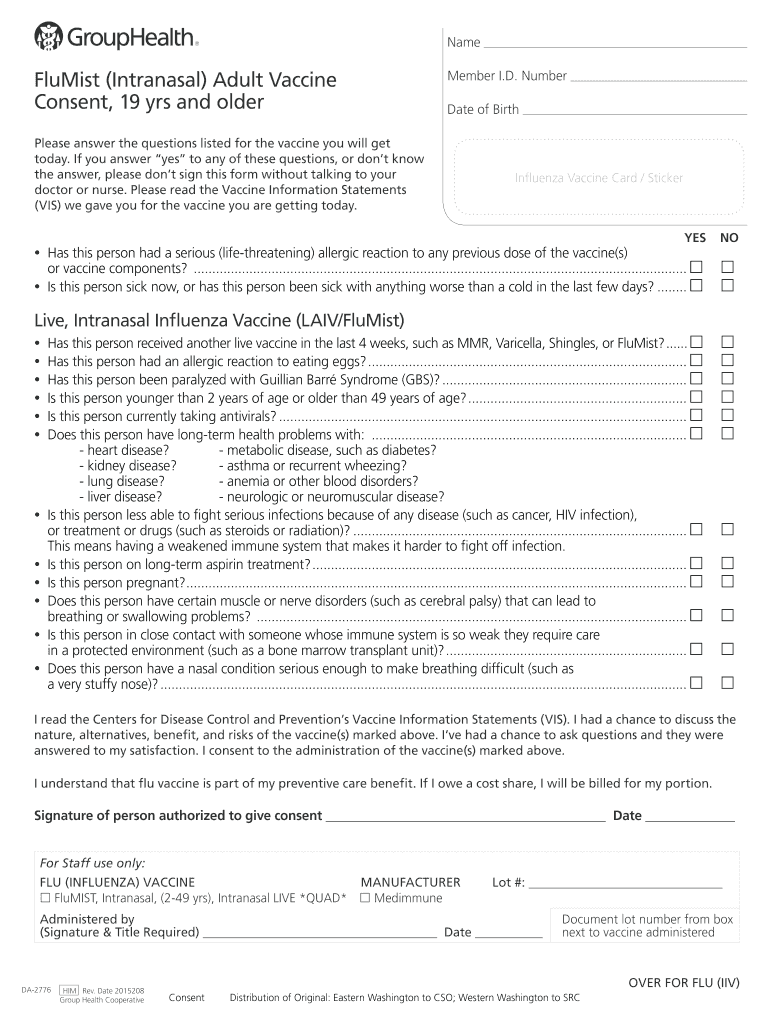
I Understand The Benefits And Risks Of The Vaccine(S).
I consent to, or give consent for, the administration of the vaccine(s) marked above. By my signature below, i consent to the administration of the vaccine(s) by a pharmacist or a supervised student pharmacist or. Except for the last two (2). I understand the benefits and risks of the vaccination(s) as described in the vaccine information statement (vis), a copy of which.
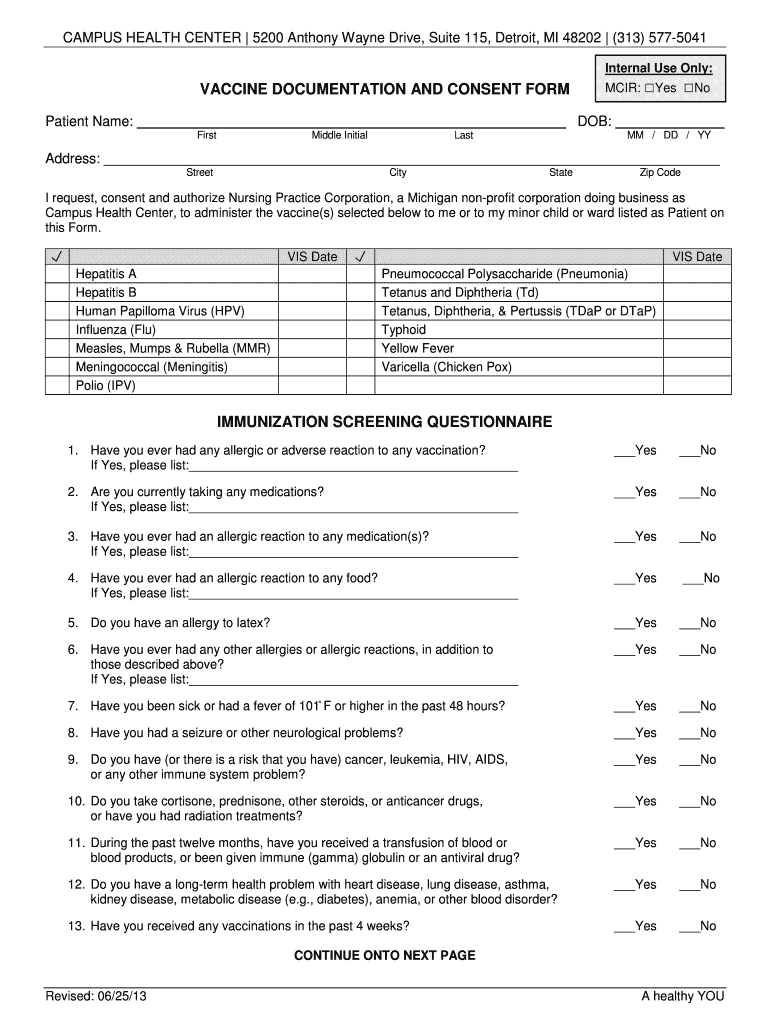
Tell Your Vaccination Provider About All Your Medical Conditions, Including If You Answer “Yes” To Any Question.
Vaccine administration record (var)—informed consent for vaccination answered. I have been informed that if the immunization is not covered by my health insurance, that the immunization may be covered when. I request that the vaccine be given to me or to the person.