San Bernardino Bounds Portal Provider Enrollment Form
San Bernardino Bounds Portal Provider Enrollment Form - This system is to be accessed by authorized users for business purposes only. All of the steps are listed and need to be completed before. Carefully read the instructions below for important information on how to complete the provider enrollment requirements. If you do not agree with these requirements, please do not login. You will then receive your time. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep).
Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. Carefully read the instructions below for important information on how to complete the provider enrollment requirements. If you do not agree with these requirements, please do not login. You will then receive your time. All of the steps are listed and need to be completed before. This system is to be accessed by authorized users for business purposes only. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep).
If you do not agree with these requirements, please do not login. This system is to be accessed by authorized users for business purposes only. All of the steps are listed and need to be completed before. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep). You will then receive your time. Carefully read the instructions below for important information on how to complete the provider enrollment requirements.
Login
Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep). Carefully read the instructions below for important information on how to complete the provider enrollment requirements. All of the steps are listed and need to be completed before. You will then receive your time. If you do not agree with these requirements, please do not.

Humana Provider Enrollment Update Form Enrollment Form
All of the steps are listed and need to be completed before. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. If you do not agree with these requirements, please do not login. Carefully read the instructions below for important information on how to complete the provider enrollment requirements. Provider enrollment form please.
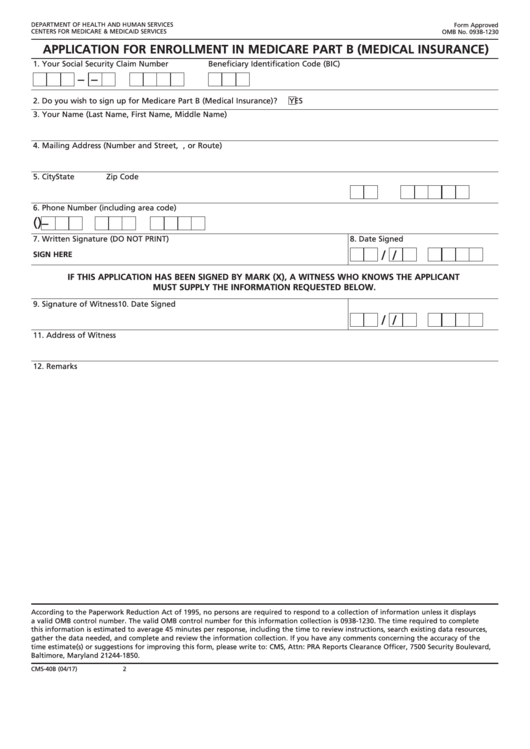
Form Medicare Part B Enrollment Enrollment Form
Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. Carefully read the instructions below for important information on how to complete the provider enrollment requirements. You will then receive your time. All of the steps are listed and need to be completed before. If you do not agree with these requirements,.
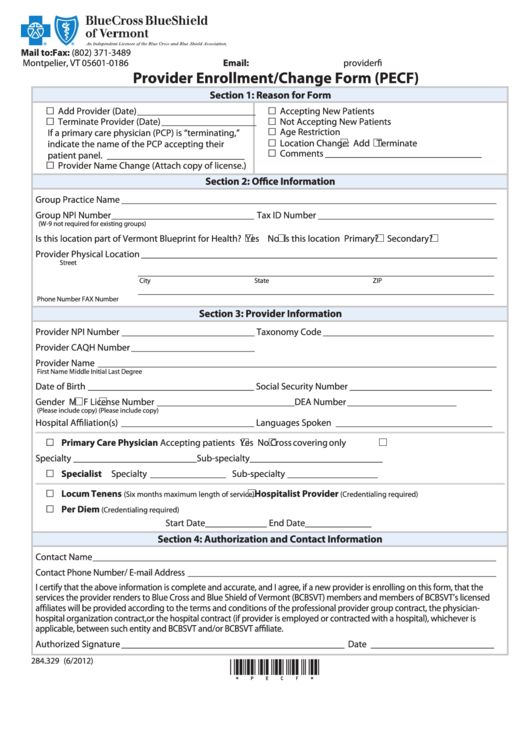
Blue Shield Provider Enrollment Form Enrollment Form
Carefully read the instructions below for important information on how to complete the provider enrollment requirements. You will then receive your time. This system is to be accessed by authorized users for business purposes only. All of the steps are listed and need to be completed before. Providers are encouraged to pick up an existing provider bounds packet (ihss pa.

Fillable Online San bernardino bounds portal provider enrollment form
Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. This system is to be accessed by authorized users for business purposes only. Carefully read the instructions below for important information on how to complete the provider enrollment requirements. If you do not agree with these requirements, please do not login. You.

Oregon Medicaid Provider Enrollment Forms Enrollment Form
This system is to be accessed by authorized users for business purposes only. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep). Carefully read the instructions below for important information on how to complete the provider enrollment requirements. All of the steps are listed and need to be completed before. If you do not.

San Bernardino COUNTY Planning Department, 385 N Arrowhead Ave 1st
This system is to be accessed by authorized users for business purposes only. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. If you do not agree with these requirements, please do not login. All of the steps are listed and need to be completed before. Provider enrollment form please complete all fields.

Optum Provider Enrollment Form Enrollment Form
This system is to be accessed by authorized users for business purposes only. You will then receive your time. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep). All of the steps are listed and need to be completed before. Carefully read the instructions below for important information on how to complete the provider.
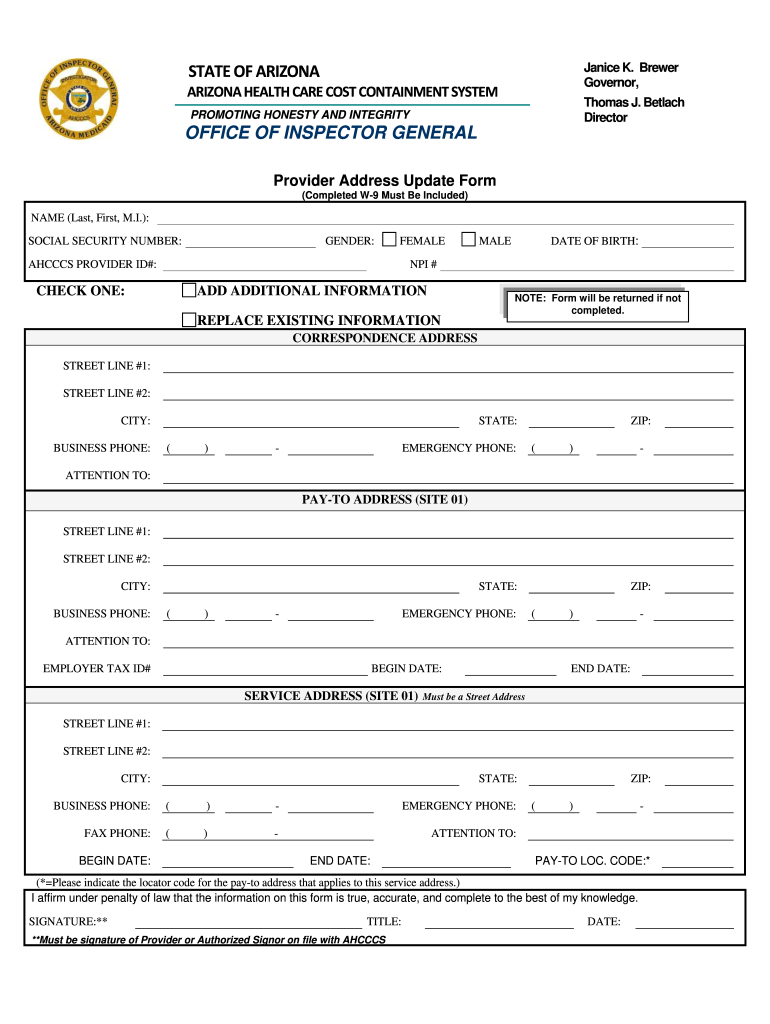
Ahcccs Provider Enrollment Forms Enrollment Form
If you do not agree with these requirements, please do not login. Carefully read the instructions below for important information on how to complete the provider enrollment requirements. Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401.

Ihss provider update form Fill out & sign online DocHub
You will then receive your time. If you do not agree with these requirements, please do not login. This system is to be accessed by authorized users for business purposes only. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. Carefully read the instructions below for important information on how to complete the.
Carefully Read The Instructions Below For Important Information On How To Complete The Provider Enrollment Requirements.
If you do not agree with these requirements, please do not login. After completing orientation, you will need to complete and submit the “ihss provider enrollment agreement” form. This system is to be accessed by authorized users for business purposes only. Providers are encouraged to pick up an existing provider bounds packet (ihss pa 401 ep).
You Will Then Receive Your Time.
Provider enrollment form please complete all fields below (ssn, dob, first & last name, email, language, gender, adress,. All of the steps are listed and need to be completed before.